Полная версия:
The Italian Reset Diet

Dario Polisano
The Italian Reset Diet
THE ITALIAN RESET DIET
THE POLISANO METHOD FOR RESETTING YOUR BODY AND IMPROVING YOUR WELL-BEING
How to lose up to 10 kg/22 lbs. in one month, and keep them off

“The Italian Reset Diet”
First Edition
Authored by Dario Polisano
Translated by Giuseppe di Martino
English edition published by Tektime
Graphics, DTP and cover:
V. Riccardo Puglisi
Images
(Book and cover):
© 2020 Dario Polisano
(Page 18):
http://www.inran.it/piramide-alimentare/9647
(Page 73):
http://www.eticamente.net/55137/in-frutta-veritas-il-fruttosio-fa-davvero-male.html
www.comidaedizioni.it
www.facebook.com/comidaedizioni
PREFACE
I am not a medical doctor, nor do I want to be. I am proud to be a nutritional biologist. My profession does not allow me to prescribe drugs or diagnose pathologies; those are tasks for doctors. I am a firm believer in our own bodies’ vital force and self-healing power. My job, or mission, is to enable that power through proper nutrition, an important factor which is, unfortunately, often underestimated.
Today’s technology helps us with innovative solutions in all fields. It also helps in the biological-nutritional field with, for example, the use of supplements, or non-synthetic molecular concentrates found in nature. A nutritional biologist can advise supplements, when essential, in order to help a patient recover more quickly. Unfortunately, often enough, what happens is that people get the mistaken idea that supplements are good for everything, without any negative effects—and that notion is absolutely false. Supplements act like actual medication. It is true that when a woman takes folic acid during her pregnancy, she avoids possible conditions such as spina bifida for her baby, but it is also true that the misuse of supplements can lead to damage instead, by causing the activation of gene mutation from its dormant to its hyperactive phase, with often disastrous consequences for our bodies. Guidance regarding the subject of dietary supplements is always best left to a conscientious and competent expert.
In this book you will also find testimonials from some of my patients, who were healed thanks to the lifestyle changes I suggested, as nutrition plays a crucial role in obtaining an optimal state of health.
Please do not misunderstand me—I am not some sort of strange quack. I just believe, as a nutritional biologist and researcher, that alongside the expertise and methodologies of a doctor who prescribes medical treatments, one must also practice proper nutrition from the very beginning of a medical condition. I assert that improper nutrition is often the root of all ills, and that healing takes more than just medical prescriptions, which more often than not hurt the development of the physical processes in our bodies. Medications are often allopathic, meaning they turn off symptoms but do not take all the side effects into account.
I would say that my method is interpretative, a sort of decoding of the signals the body sends in order to try to find balance and promote self-healing. This way, the value-ranges will tend to improve, and once a physician sees that the patient is getting better, he or she may reduce the medications. And why not? He or she may even do away with them altogether.
This is often not appreciated by those doctors who do not see a link between healing and proper nutrition. Often patients are even laughed at by their own physicians for this, thus causing them to have a real psychological crisis to the point of doubting the food choices recommended by the nutritionist. Those doubts are quickly done away with by patients when, by going back to their old way of eating, they see that their old symptoms, which were maybe either totally gone or at least kept at bay with a proper food regimen, show up again.
I have often been accused of being a charlatan, but results are what matter. You will surely have noticed that I am slightly argumentative, but I believe that, when it comes to evidence and concrete results for your health, by being argumentative in a constructive way, it helps to put in question the claims certain experts make.
These are situations that truly occur every day. Many of my patients are told by their doctors to interrupt the food regimens I suggested for them, even though they see positive results. I consider this sort of professional rivalry useless and damaging, and I always ask myself why we cannot walk hand-in-hand to reach common goals.
I am always willing to cooperate with doctors for the exclusive benefit of the patient, but I rarely receive the same courtesy. I could go on and on about the medical professionals who never took into consideration what their patients told them, even when they described the benefits of a personalized diet, and who asked themselves why they had to settle for the temporary effects of drug treatments, without receiving any answer.
I want to clarify that drugs were no doubt a very important discovery, but they are often used when there is no need. It is normal practice for a doctor to prescribe something immediately, as soon as they see a value out of range, without caring to know what the patient eats. They do not even consider that those values can go back to a normal range through a proper diet. This happens because a drug prescription is sometimes the fastest way of seeing results, but trust me, they will not be long-lasting. Sooner or later, the body will manifest other symptoms and the onset of another illness. This is when patients will find themselves taking up to 6-8 different types of medication a day.
My polite yet resolute position does not salvage the “Mediterranean Diet,” the one discussed daily on TV or read about in magazines or on the Web, which is totally different from the original Mediterranean Diet. For some experts, it is enough to eat bread and pasta for them to say that you are following the Mediterranean Diet. For example, I have seen diets where a gentleman was advised to eat white bread and creamy cheeses for lunch by his doctor, who objected to and criticized some of my dietary recommendations (which included legumes and fish).
On the other hand, I can say that, out of intellectual honesty, often on my career path I have encountered doctors and colleagues who appreciated my work very much and trusted my intuition and foolproof scientific evidence, so much so that they entrusted those who were dearest to them (wives and/or kids) under my care.
I will also tell you, briefly, what happens inside a nutritional biologist’s office, where we look for the most suitable solution to improve a patient’s state of health, even in the presence of discouraging news.
I have seen obese people with sky-high glycemia continue to eat ready-made food or food made with white flour every day, pushed by their own doctors to go back to their old diets which they deemed reliable, because mine did not follow the standards of the hypothetical “Mediterranean Diet.”
I am a simple, social and honest person who has never had an agenda, ulterior motives or monetary interests, especially when it comes to health. I will try to explain to you not only my truths as a nutritional biologist, but also the everyday objective truths regarding health problems.
My food system is not called the Italian Reset Diet for no reason; the word “reset” has a specific purpose—to reset your body gradually and bring it back to proper nutrition in a controlled manner. Justifiably, you may now be thinking that all of this is based on dietary deprivation and constraints, but you will change your mind once you have read the last part of the book, which is about how you have at your disposal an infinite variety of food products typical of the peoples who have lived in our Italy: eggs, legumes, fish, seasonal fruits, ancient whole grains and much more.
My method does not want to replace conventional medicine, but it should work side by side with it, guaranteeing, at worst, an improvement in the patient’s quality of life and a reduction in drug treatments, and at best—something not rare if an illness is caught in time—complete healing.
INTRODUCTION
My journey as a therapist began in early 2011. At the time, I was a young man studying Pharmaceutical Science at the University of Messina. I was then, and still am, a great sportsman, but back then I did not have my current professional knowledge.
As often happens with athletes, I made serious nutrition mistakes. I trained four times a week to gain muscle mass, and was a big consumer of high-quality protein, derived from milk and cheeses: caseins. I drank more than 1 liter of milk every 24 hours. As a matter of fact, thanks also to my genetic predisposition to building lean muscle mass instead of fat, I soon saw results: 10 kg (approx. 22 lbs.) of lean muscle mass in six months, impressive numbers in the eyes of any personal trainer. Unfortunately, the muscle mass came with my first organic disorders.
One evening, around 10 pm in January 2011, I was sleeping at home in Messina, when I suddenly woke up to a violent intestinal colic. Alone, frightened and panicking, I did not even think to go to the emergency room; I remained there for hours with that devastating intestinal colic. Early the next morning, around 4 am, exhausted by the pain, I called my parents, who, frightened, rushed over almost immediately from Caltanisetta. It took a two-and-a-half-hour car ride for them to arrive, and they immediately took me to the city hospital’s ER while I was almost unconscious from the pain and violent spasms. The health protocol applied there was symptomatic treatment: painkillers, antispasmodic drugs and antacids.
From that day on, the attacks hit me weekly and grew more and more intense: toxic states characterized by nausea, diarrhea and vomiting. At night I slept pretty poorly; my nasal turbinates were always irritated and swollen, and my doctors were pushing for a surgical solution. Plus, I had cervical pain and vertigo all the time. No one could explain to me the cause of my ailments, and oddly, we talked about everything except for nutrition.
Despite these debilitating issues, in March 2013 I earned my degree and decided to take six months off before continuing my studies. I always thank fate and my tenacity for taking that free time, which I used in the best possible way—by trying to understand and resolve my health issues. Clicking away at my mouse, my battle to take back control of my health began with the discovery of Dr. Piero Mozzi’s diet. In just a few days, I regained control of my health almost 100%: no more vertigo, no more toxic states, an exponential increase in muscle strength (which had been previously diminishing), and the total disappearance of my nasal swelling and migraines. I came to understand the great power of food, this secret medicine no one had ever told me about, and that I myself, a fanatical Pharmaceutical Science student, had ignored. The only remaining problem was my irritable bowel syndrome, which was somewhat under control without any real colics, but ever-present with the changing of the seasons, or any type of mental or physical stress. I began a new course of studies in “Food Science and Human Nutrition” as passionately as a fanatic of the blood type diet, but the desire for knowledge inspired me to search for all those food molecules that led people, especially one’s loved ones, to a bad state of health.
I embarked on an endless search of all existing diets: macrobiotic, vegan, Kousmine, paleo, etc. I asked questions to people on particular diets in order to understand the various health issues they had resolved. I found myself with thousands of pieces of data to cross-reference where people, though on very different diets, managed to resolve their problems anyway. What was the least common denominator that allowed these people to resolve the same issues with totally different diets? Despite my study work load, and the time I needed to devote to it, I still managed to find the time for my research: nighttime. I will admit that I went a bit overboard for a while, but I noticed that by eating correctly, I was able to overcome any stressful event. I graduated in 2015 and started to work, and through gathering accurate medical histories on my patients, the data became clearer.
CHAPTER 1
THE “HEALTHY” MEDITERRANEAN DIET
Premise
The end of the Second World War was a very important and significant event in the history of mankind. Other than redistributing the population map of the West, in the early post-war period (around 1950), a true food revolution began to put strain on our bodies. The human body functions like a well-oiled machine, but when atypical dietetic conditions occur, it needs time to make the best of these new conditions. Yes, our genes do not mutate easily; it takes thousands of years for significant change in the human genome. When we input something in our immune system that is not recognized, the body does not work properly. It is up to us, maybe with the help of a nutritional biologist, to bring everything back to normal.
The consequences of this food revolution presented themselves almost immediately. In fact, from 1950 to today, numerous new pathologies have appeared, and they are putting the best researchers in the pharmaceutical field to the test. We used to fight bacterial infections; today these are gone, making way for metabolic, tumoral and autoimmune diseases, whose causes they say are unknown. To name just a few: type 2 diabetes is affecting 246 million people, and in Italy alone there are 6 million patients with thyroid dysfunctions. In addition, there are 3 million people with multiple sclerosis, and 1,000 tumor cases are discovered in Italy every day. We could go on and on with these dismal statistics, but better to stop and make sense of it all. Despite these frightening data, we continue to believe that medicine has taken several steps forward and that life-spans have increased; honestly, I do not believe that it is anyone’s dream to live to 85 if it means being a depressive slave to ten medications, with fewer organs than before and with an inability to walk autonomously. Do you? I really do not think so.
Even today, we continue to ignore the close connection between the explosion of illnesses and the aforementioned food revolution—on the contrary, we are constantly invited to follow the “healthy Mediterranean Diet,” recognized ever since 2010 as being on the Representative List of the Intangible Cultural Heritage of Humanity by UNESCO. The consequences of these facts are devastating: I find myself in the office writing up food regimens for children with fatty livers, and rebalancing the bodies of adolescents dealing with the onset of lupus erythematosus, psoriasis, and various autoimmune diseases. What saddens me the most is that every day, when I ask new patients about their medical history upon their preliminary analysis, many of them sit down and say that there is nothing wrong with them. Considering their (maybe even a tad advanced) age, I find myself insisting they reflect on their condition:
Me: “Ma’am/Sir, are you sure you do not have any ailments?”
Patient: “No, doctor, I’m sure.”
Not convinced, I ask the customary question:
Me: “Are you on any medication?”
Patient: “I only take a pill for my diabetes and one for my blood pressure.”
It is moments like these that clue me into how much the average Westerner is used to relying on drugs, and to being in constant contact with diseases—so much so that they are considered a part of us. More depressing still, after reprimanding them for neglecting their own health, I often hear: “Doctor, if you call these illnesses…” or “I take the pill and I’m fine.” It is then that I understand that it is not really their fault, but rather society’s. Society does not facilitate the spreading of health awareness. Eastern populations, though not as technologically advanced, have an inherent respect for their own bodies. In Japan and India, for example, they live using natural treatment methods for their bodies and minds, which are methods available to all, and that are inculcated in them since childhood. Health education and respect for our own bodies are the really important things in this life. We should consider ourselves lucky that our conscience or spirit, (depending on one’s beliefs), came to be in a healthy body. And yet what do we do instead? We destroy our cells with the crap that is offered us every day. Adults, with their food miseducation—but even worse, with their arrogant assumption that they are perfectly able to safeguard their children’s health—convince their kids that the products they are consuming are the best for keeping in shape. Chocolate and candy are the rewards for children who receive good grades or who do well in class. Holidays, religious or not, are a pretext for preparing lavish meals where the majority of guests, as soon as the guest of honor appears, fling themselves toward laden trays of food that is anything but natural. Sometimes we are so fixated on the food that we forget even to congratulate the honoree. And what kind of a party would it be if it did not end by gorging on sweets?
How the “Mediterranean Diet” Is Presented
She is the great media starlet, the “healthy” and historic “Mediterranean Diet.” On all public TV stations, there are exciting little stages where many professionals, supporters of the Mediterranean Diet, are invited. They all line up against the ill-fated nutritionist who, in accordance with his own work experience, found all of the holes in what is today listed as an Intangible Cultural Heritage element: the “Mediterranean Diet.” These little panels do nothing but confuse those people who, when in doubt, fall into theoretical “Do It Yourself” health paths, listening to a variety of canards such as “red meat causes tumors,” or “alkaline diets are miraculous,” or “carbohydrates constitute the main energy source of cells,” or “drinking lemon water in the morning cleans the overnight accumulation of mucus out from the intestines,” etc. The result? When these people convince themselves to come see me at my office, I have to resolve both the problems created by the hypothetical “Mediterranean Diet” and those caused by the “miraculous” alternative theories patients came across online.
As an occupational hazard, in addition to taking a patient’s medical history and asking in detail about their daily food habits, I tend to observe the food carts of patrons at the supermarket. Over the course of time, a thought has isolated itself in my mind, detached from all that was narrated to me during my study courses and during nighttime channel surfing, and I have come to the conclusion that it is the hypothetical “Mediterranean Diet” that has created this health crisis in the Western populace. Easy now—I too may be taken for a witch doctor by a couple of professionals who back the Mediterranean Diet, but no matter. The time has come to tell you what a “healthy” Mediterranean Diet is, and above all, how it came about. In time, you will come to understand how science, because of an affirmation typically inherent to its “scientific” research, manages to deceive itself and the rest of the population.
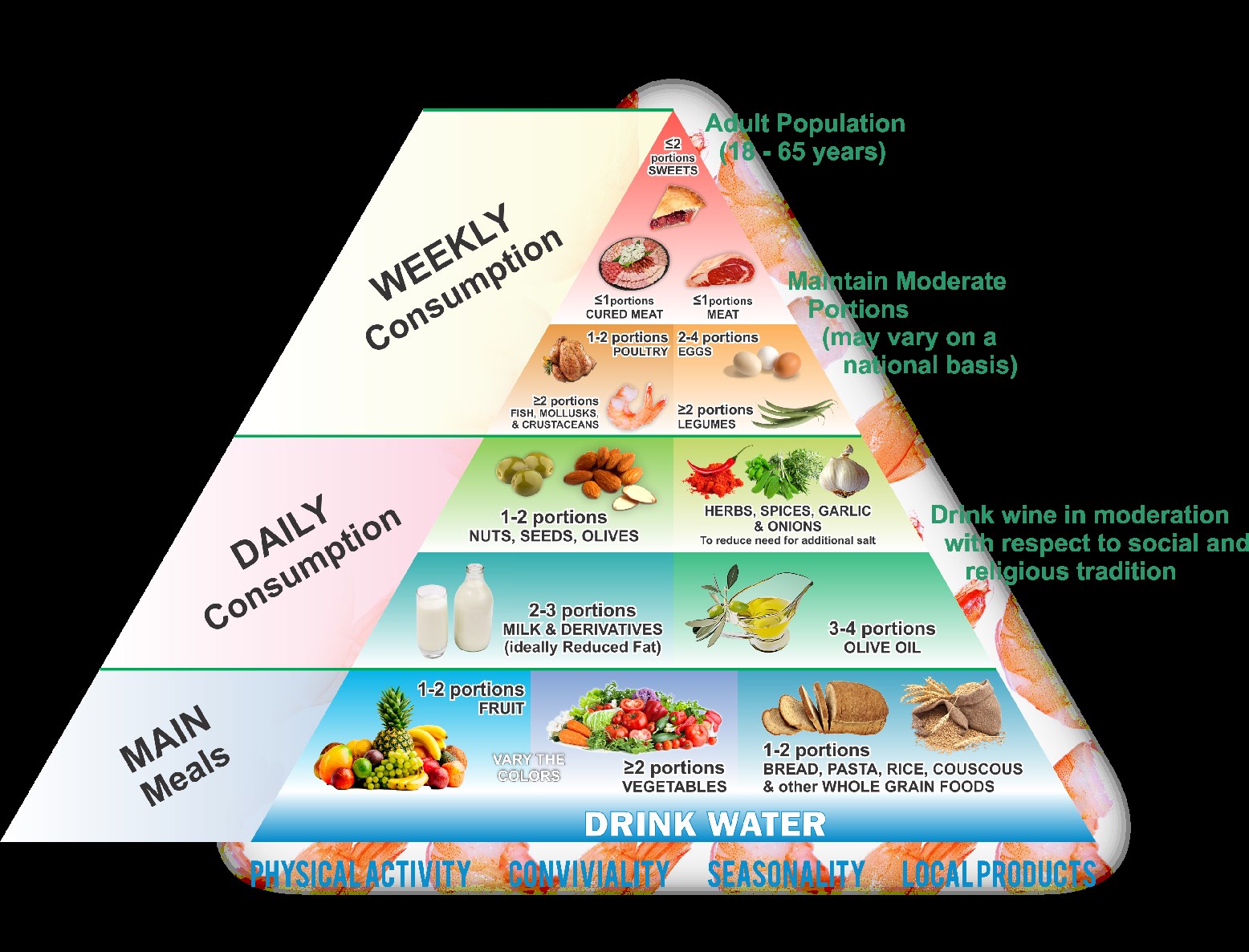
They tell us that the “Mediterranean Diet” is the food regimen that is been followed by the people who bordered the Mediterranean Sea, where the climate allowed many species of plants to grow for thousands of years—from vegetables to cereals and legumes. The great study that led to the discovery of the benefits of the “Mediterranean Diet” was made by an American researcher by the name of Ancel Keys, who, together with his team, came to Italy and a few other countries adjacent to the Mediterranean to figure out why cardiovascular diseases were almost non-existent in these specific areas. Ancel Keys’s team studied how these people ate, and were immediately astonished: the Mediterranean people, who had almost non-existent cardiovascular diseases, consumed lots of fats, primarily via eating dry fruits and most especially extra virgin olive oil. Keys continued his studies and concluded them with what is currently presented to us as the healthiest diet in the world: the “Mediterranean Diet.” The diet is represented by the famous food pyramid that shows, at the very first and largest bottom step, what people should eat the most, and, alas, consume as their main meals: cereals (wheat, rice, oatmeal, etc.) and fruits and vegetables. Therefore, cereals are recommended for breakfast, lunch and dinner. Yes, you heard that correctly: even after getting home at night, we should apparently be eating our beloved bread, in deference to one theory—the theory of the scale—which claims that it is quantity which creates health problems. Maybe, I say, but not in this case. What results is an obsessive compulsion (which turns into an actual mania) to weigh everything at all costs, with overly exact and expensive little food scales used to try to avoid an extra milligram of cereal.
As you will see in the following pages, I describe the consumption of carbs at night as a veritable bonanza for diabetes. And if this were not enough, we are even advised to consume the simple sugars found in fruit. But we will go over this in the following chapters. In my opinion, the horror of the diet they pass off as Mediterranean lies in the encouragement of the daily consumption of dairy because they say Mediterranean people consumed it during every meal.
Luckily, Italy’s extra virgin olive oil is also recommended for daily consumption. On the highest tier of the food pyramid we find meat, shellfish, eggs, legumes and seafood. Eggs, legumes and seafood on the last tier, together with meat? Mediterranean people really only ate fish twice a week? And legumes?
The “Mediterranean Diet,” in percentages, calls for the total daily calorie intake of carbs to be 55-65% (of which 10% is from simple sugars, thereby encouraging the consumption of glucose and fructose); 25-30% of calories in the form of fats, and the rest, (meaning a max of 15%), from proteins. Proteins are demonized together with fats as being harmful to one’s health. That is how you have the whole population flinging itself onto carbs and cereals for years, and glutinous grains in particular, which are anything but healthy. There is usually an argument whenever a patient, under the care of this pseudo “Mediterranean Diet,” substitutes wheat pasta with buckwheat pasta; he or she is declared reckless and gullible by his or her own physician for daring to consider ordinary pasta, (and white and refined pasta at that), the cause of his or her problems. Yet, just so we understand each other, buckwheat pasta has the same amount of carbs as ordinary pasta but of a different quality, and when you hear the physician whose care you are under for your food regimen, and who often specializes in everything but nutrition, say that a diet without carbs is a health risk, you ask yourself: “what do you mean, without carbs?” Surely, that physician has never read the nutritional value of buckwheat—otherwise he or she would not be making statements lacking any sort of knowledge in nutritional biology. Who is left picking up the bill, then? It is the poor patients who often find themselves almost forced to leave it to fate and flip a coin for advice on the right path to follow. Heads: “I’ll listen to the potbellied physician who suffers from diabetes.” Tails: “I’ll try this new theory by this fit young physician who has resolved his own health issues simply by consuming specific categories of food.”
What Was the True “Mediterranean Diet”?
Dear friends and readers, the true “Mediterranean Diet” dates back to the Greeks and the Romans, populations that shared the areas by the Mediterranean Sea. Surely, in those days, there was no physician on duty who recommended the proper food amounts each person needed to eat in order to maintain their ideal weight, or to optimize their health. People ate when they were hungry and, among the poorer echelons, whenever food was available. The cultivation of cereals existed back then too, but luckily for them, agriculture was not as intensive and the consumption of grains was limited to the period from July to December, (if there was a great harvest). For the rest of the year, people’s main meals were based on legumes and wild vegetables, and they ended with dry fruits/nuts. As for the dressing? Extra virgin olive oil.

