Полная версия:
Model for Integral Assessment of Students’ Physical Health. Teaching and Methodological Manual

Model for Integral Assessment of Students’ Physical Health
Teaching and Methodological Manual
Arsentiy Aleksandrovich Krasilnikov
Translator Feliks Khaidarovich Zakirov
© Arsentiy Aleksandrovich Krasilnikov, 2023
© Feliks Khaidarovich Zakirov, translation, 2023
ISBN 978-5-0060-0300-2
Created with Ridero smart publishing system
From the author
Dear Readers,
I am pleased to present my latest monograph entitled «Model for Integral Assessment of Students’ Physical Health» This methodological guide serves as an extended additional material for the course «Theory and Methodology of Physical Education» in all Bachelor’s and Specialist programs.
The educational and methodical material provided in this guide is highly relevant for developing new competencies among students in the field of building independent physical education sessions, maintaining an optimal training regime, and forming the basics of a healthy lifestyle. It contains theoretical material that, when studied, will contribute to increasing the effectiveness of developing students’ competencies in the field of a healthy lifestyle, assessing the functional state of organs and systems of the body, and a comprehensive assessment of the level of health.
I hope this guide will be useful to students and teachers of higher educational institutions, physical education teachers, and specialists in the field of physical education and sports.
Best regards,
A. A. Krasilnikov
Introduction
Health is one of the fundamental values in life, and it is unlikely that there is anyone who would say that they do not want to be healthy. However, wanting to be healthy is not enough, as maintaining good health requires constant self-improvement, leading a healthy lifestyle, following the rules of rational nutrition, hygiene, and of course, properly organized physical activity.
Medical and sports science has proven that physical training through exercise increases the functional abilities of the body by increasing the functional efficiency of muscle cells and the oxygen transport system.
However, not every physical activity can be beneficial. Uncontrolled use of means of physical culture and sports can not only lead to undesirable consequences but also harm one’s health. Therefore, self-monitoring plays a significant role in this issue.
Self-monitoring is the regular monitoring of individuals engaged in physical culture and sports of their health status, physical development, functional and physical preparedness, using various publicly available techniques and methods.
During self-monitoring, externally set «norms» are transferred into the sphere of personally significant norms, and the dynamics of changes in all indicators are tracked, which provides feedback and serves as a stimulating factor for starting active physical exercises.
Section 1. Self-evaluation of physical development indicators
Research related to the assessment of physical development is conducted using various anthropometric techniques:
1. somatometric – body length (height), body mass (weight), chest circumference and excursion;
2. physiometric – vital lung capacity (VLC), hand grip strength, standing strength;
3. somatoscopic – chest shape (body type), posture and so on.
IT IS IMPORTANT TO KNOW THAT!
Physical development of a person is understood as a complex of functional and morphological properties of the body that determine its physical ability. Physical development can be influenced by:
heredity; environmental conditions; socio-economic factors; working and living conditions; nutrition; physical activity; sports.
There is no clear boundary between normal and pathological conditions. There are various transitional stages between health and illness. Disease usually occurs when the body is subjected to excessive physical and psycho-emotional stress or when adaptive functions are decreased. This is when changes occur, often leading to illness or injury.
Norm in relation to human health is interpreted as the measure of the organism’s vitality in specific environmental conditions, within which changes in physiological processes are maintained at an optimal level of functioning of the homeostatic self-regulation.
It is important to note that the norm in relation to the human body does not have a single value. Biological norm has certain boundaries. Thus, the norm is such an indicator at which the human organism functions in the best way possible (i.e. in an optimal mode). At the same time, a healthy organism is able to maintain normal indicators of its functions in various situations (physical exertion, psycho-emotional stress, weather changes, etc.). This property of the organism is called adaptation. It is adaptation that helps a person to maintain the functioning of organs and systems in a normal state and to preserve health in various stressful situations.
It should be noted that the reduction of the adaptive capacity of the organism is associated with changes in physiological functions. This is characterized by an increase in blood pressure and a decrease in heart activity. However, in pre-disease states, the observed changes in physiological indicators, as a rule, do not exceed the so-called clinical norm and therefore usually remain outside the field of view of doctors during dispensary and preventive examinations of the population. As a result, only a disruption of adaptation with the development of specific diseases becomes the basis for therapeutic measures.
Disease is the destruction of the normal state of a living system, the transition of it to a new altered state, in which the indicators of organs and systems deviate significantly from the norm. If special therapeutic measures are not taken in this state, the disease can become prolonged and chronic, and the organism can ultimately perish.
Somatometric indicators
When assessing the somatometric indicators of an adult’s physical development, the values of various indices that evaluate the ratios of height and weight, height, weight, and chest circumference are more important. The most well-known indices include the Kettle index, the Pignae index, the BMI – body mass index, and others.
Body Mass Index (BMI) is a value that allows evaluating the degree of correspondence between a person’s body weight and height, and thus make a conclusion whether the weight is insufficient, normal, or excessive. BMI = body weight (kg) / height (m2).

Table 1. Interpretation of BMI values.
The Body Mass Index (BMI) is a measure that allows evaluating the degree of correspondence between a person’s body weight and height, and thus draw conclusions about whether the weight is insufficient, normal, or excessive. The BMI is calculated as body weight (kg) divided by height squared (m2).
It should be noted that the BMI should be used with caution, solely for approximate assessment. For example, attempting to assess the body composition of professional athletes with its help may give a false result (a high index value in this case is explained by developed musculature). The ideal BMI for men is between 25—27, and for women between 23—27.
In the context of the above, it is important to remember that both excessively high and low weight should attract your attention.
Most often, obesity occurs due to excessive consumption of high-calorie food containing large amounts of fats and carbohydrates, while the person’s physical activity is sharply reduced. Such obesity is called primary or alimentary. The most effective treatment for primary or alimentary obesity is diet and physical exercises.
There is also obesity that occurs due to various diseases of the endocrine glands and the central nervous system. It occurs much less frequently and is called secondary. Such obesity requires special treatment by a doctor.
Obesity can cause diseases of the cardiovascular system, gastrointestinal tract, genitourinary system, respiratory system, endocrine glands, joints, and spine.
Decrease in body weight can lead to weakening of the body’s resistance to diseases, a decrease in the level of vital energy with nervousness and insomnia, poor appetite and depression, general malaise, and mental instability. Tissue depletion can be accompanied by signs of premature aging with hair and tooth loss, and bone fragility. Insufficient weight (excessive thinness) can be considered a disease if the weight is significantly reduced and predisposes to the disruption of the heart, kidneys, blood vessels, tuberculosis, and other diseases, as well as in the terminal stages of tumors of various organs.
IT IS IMPORTANT TO KNOW THAT!
the human body cannot exist without oxygen, which is obtained from the surrounding atmospheric air, containing about 21%. At the beginning of the oxygen delivery process to the body is the respiratory system, which through respiratory movements of the chest carries out ventilation of the lungs. Breathing essentially represents gas exchange between the body and the external environment. The final stage of breathing is the utilization of oxygen by tissues and their release of CO2. Breathing is a set of processes that provide the body with oxygen consumption and the release of excess carbon dioxide, aimed at maintaining the body’s gas homeostasis. The respiratory system begins with the nose and throat, followed by the trachea and two major bronchi for the left and right lungs. Then, the bronchi divide dichotomously, i.e., each one into two daughter bronchi, with a total of 23 generations of the bronchial tree. Under resting conditions, a person breathes in such a way that only a part of the total lung volume is used, so there is always a reserve for inhalation and exhalation. Four lung volumes are distinguished: Tidal volume (TV) – the amount of air that enters the lungs with each inhalation; Inspiratory reserve volume (IRV) – the amount of air that a person can additionally inhale after a normal inhalation under resting conditions; Expiratory reserve volume (ERV) – the amount of air that a person can exhale after a calm exhalation; Residual volume (RV) – the amount of air that remains in the lungs even after the deepest exhalation (Figure 1).
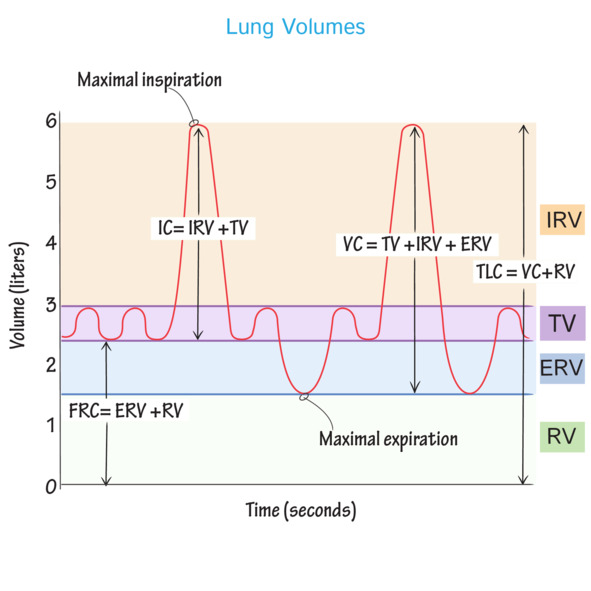
Figure 1. Pulmonary volumes and capacities.
According to the commonly accepted classification, primary lung volumes are combined into so-called lung capacities, of which there are also four. The most commonly used in practice to assess a person’s physical development is the vital capacity of the lungs (VCL) – the amount of air that can be exhaled from the lungs after a maximum inhalation. VCL consists of three volumes: VCL = tidal volume (TV) + inspiratory reserve volume (IRV) + expiratory reserve volume (ERV).
1.1. Assessment of physiometric indicators
Vital Capacity (VC)
The normal value of VC depends on the person’s gender and age, body type, physical development, and may significantly decrease in various illnesses, reducing the body’s ability to adapt to physical stress.
In men, the normal VC is calculated at 60 milliliters per 1 kilogram of weight for non-athletes and 65 milliliters or more for athletes, while in women, it is 50 and 55 milliliters, respectively. The average VC is about 2.5—4 liters for women and 3.5—5 liters for men. Absolute VC values are not very informative due to individual variability. It is recommended to calculate «due» values when assessing the condition.
Calculation of the predicted lung capacity (PLC) in liters:
PLC for men = 5.2 x H – 0.029 x A – 3.2
PLC for women = 4.9 x H – 0.019 x A – 3.76
H – height in meters, A – age in years.
The actual lung capacity is considered reduced if it is less than 80% of the PLC. Lung capacity indirectly reflects the size of the respiratory surface of the lungs, where gas exchange occurs between alveolar air and blood in pulmonary capillaries. In other words, the larger the lung capacity, the greater the respiratory surface of the lungs. In addition, the larger the lung capacity, the deeper the breath and the easier it is to achieve an increase in ventilation volume. Thus, lung capacity determines the ability of the body to adapt to physical exertion, to a lack of oxygen in the inhaled air (for example, when ascending to altitude). Lung capacity is an indicator that largely determines the functional capabilities of the external respiratory system. A decrease in lung capacity always indicates some pathology. Lung capacity cannot and should not be considered the only indicator of increased function of the external respiratory system. It only determines the functional capabilities of this system in terms of providing the body with the necessary amount of oxygen. Therefore, the potential capabilities of the external respiratory system in a person with high lung capacity are higher (larger respiratory surface and the ability to deepen breathing) than in a person with low lung capacity.
Recommendations for low JEL levels:
1. During the learning process: frequent ventilation of the room and physical activity during breaks aimed at working the main and auxiliary respiratory muscles.
2. Increase time spent in forest-park zones. Reduce or eliminate harmful habits such as smoking, as this leads to a reduction in the synthesis of surfactant on the inner surface of lung alveoli, which prevents their collapse.
3. Include complete proteins and fats in the diet that restore surfactant in lung alveoli.
4. Include daily aerobic physical activity, outdoors for at least 30 minutes. Use types of motor activity that train the respiratory system according to personal choice. Include various breathing exercises.
5. Keeping health diaries to monitor daily routine, training, and body condition.
Hand Muscle Strength
Normally, the average strength of the right hand muscles (for right-handed individuals) is 35—50 kg for men and 25—33 kg for women. The average strength of the left hand muscles is usually 5—10 kg less than that of the right hand.
Any measure of strength is usually closely related to the volume of muscle mass, i.e. body mass. Therefore, when evaluating the results of dynamometry, it is important to consider both the main absolute strength (i.e. the value shown by the dynamometer) and the relative strength, i.e. relative to body mass. Relative strength is expressed as a percentage. To calculate it, the value of the strength of the right hand is multiplied by 100 and divided by the body mass value. Decreased strength can occur due to illness, negative mood, fatigue, disruption of the motor mode, aging, etc.
Конец ознакомительного фрагмента.
Текст предоставлен ООО «ЛитРес».
Прочитайте эту книгу целиком, купив полную легальную версию на ЛитРес.
Безопасно оплатить книгу можно банковской картой Visa, MasterCard, Maestro, со счета мобильного телефона, с платежного терминала, в салоне МТС или Связной, через PayPal, WebMoney, Яндекс.Деньги, QIWI Кошелек, бонусными картами или другим удобным Вам способом.
Вы ознакомились с фрагментом книги.
Для бесплатного чтения открыта только часть текста.
Приобретайте полный текст книги у нашего партнера:
Полная версия книги
Всего 10 форматов

